:format(webp)/cdn.vox-cdn.com/uploads/chorus_image/image/35294140/112868231.0.jpg)
Lots has been written about how high health care costs in the US are, and how mediocre outcomes are relative to those high costs. The American Health Care Paradox: Why Spending More Is Getting Us Less offers a new way of looking at the issue.
Health reform efforts have emphasized health insurance and medicine, sidelining social service programs like nutritional support and housing assistance — programs that can be influential for keeping people healthy and producing health, instead of just reacting when people fall ill, like the health care system often does.
Ignoring the social side of health is a problem, and it's a problem that's been plaguing the United States for decades.
Elizabeth Bradley, a professor at Yale University, and Lauren Taylor, a Presidential Scholar at Harvard Divinity School, examined this at length in their book. I spoke with the authors about the issues they see in the current system, what lessons we might draw from other nations, and what policymakers should think about next.
What follows is a transcript of our conversation, edited for clarity and length.
Adrianna McIntyre: Can you start by summarizing the core message in your book — what is the "paradox" in American health care, and how do you start to unravel it?
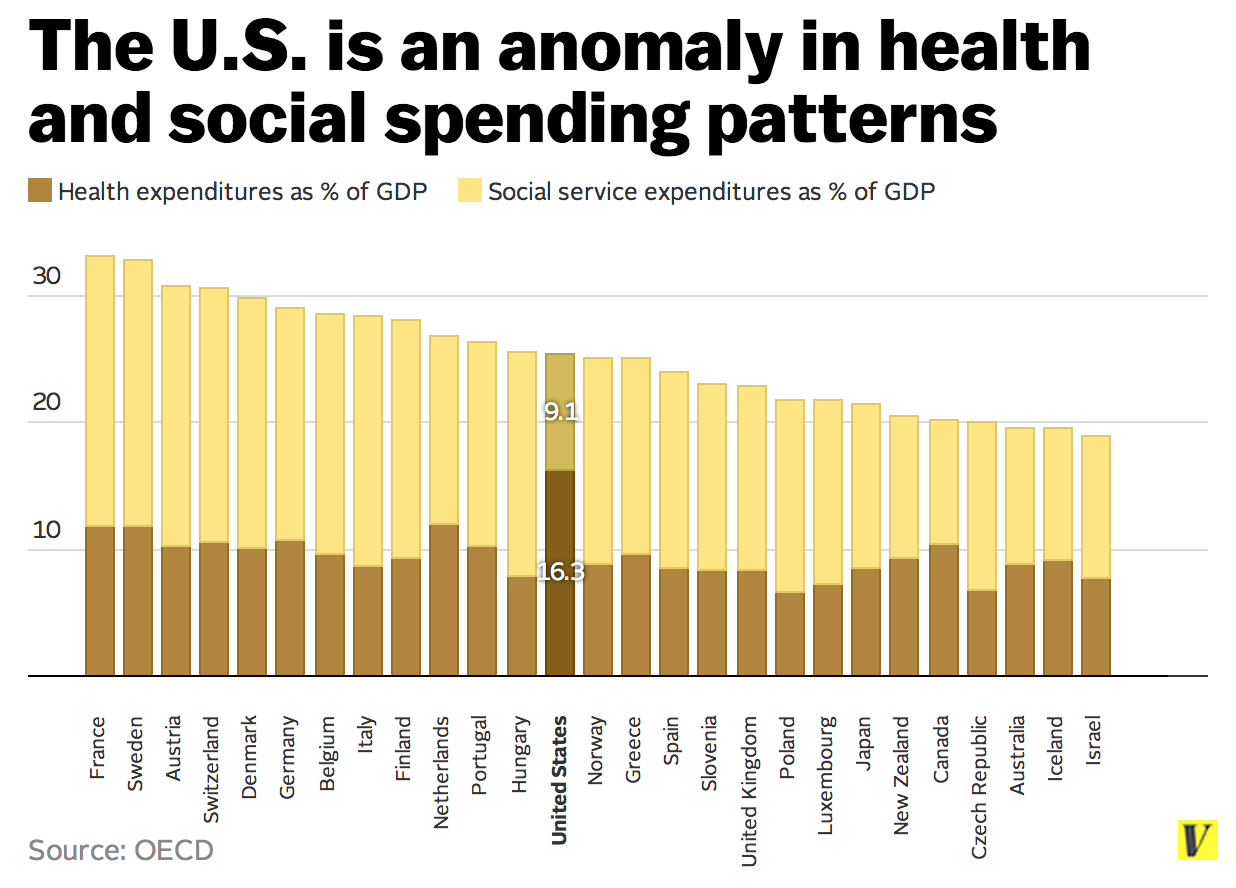
Lauren Taylor: The paradox that we outline is one that a lot of readers will be familiar with: that the United States has very high health-care costs, and in many cases middling — and sometimes lousy — health outcomes when you look at certain metrics. These are metrics — like infant mortality and life expectancy — where, when you look across developed nations, we're really at or near the bottom.
People cited this paradox before our book, and tried to explain it in any number of different ways. That included rationales like, "Well, U.S. health outcomes are bad because too few people have insurance" or "because prices are just high."
What our book tries to do is offer another reason that hasn't been talked about much in health policy: maybe "health spending" isn't telling us the whole story. Maybe we need to look at a broader summary of what resources nation puts in to support population health.
To do this, we included social services spending in our study, which captures things like housing, food assistance, and job training. The ratio of health to social-service spending was more predictive of several outcomes than health spending alone. This led us to suggest that social-service spending — and, more broadly, attention to the social determinants of health — could be a missing piece in the health reform discourse.
AM: This all started with a New York Times editorial that you two co-authored, and the preface of your book talks about the title of that editorial. Can you explain why To Fix Health Care, Help the Poor is overly simplistic?
Elizabeth Bradley: As the writer, you don't select the title; the editor does. While we were delighted that the New York Times wanted to cover this, the title made us step back a bit.
That title laid this whole problem at the feet of "the poor." In some ways, I think that narrowly portrayed our work as implying that this is all about people who are low-income. It suggested that if we could get those people — people who are homeless, drug users, the unemployed — if we could fix that piece, we would be done.
Although that is clearly important, our point is broader than that. The root of the problem we're talking about applies to the middle-class, the upper-middle class, to everybody.
Think about shoulder pain or back pain. It's very common in the American public to think "What kind of MRI do I need? What kind of specialist should I go to?" as opposed to thinking "Hm, maybe the briefcase I've been carrying around is too heavy. Maybe I'm not sleeping well. Maybe I haven't hit the gym for the last three weeks."
The issue of not appreciating the non-medical side of health plays itself out in all levels of our society. It's just that when you're middle-class or upper-middle class, you can afford to pay out-of-pocket to resolve these problems. When you're in a lower income bracket, that sometimes falls to the state.
To address the problem of over-medicalization of health we need to actually get to the way people relate to their own health, no matter how wealthy they are.
AM: You interviewed dozens of professionals who work in both health care and social services sectors for this book, and you say that the message you heard from them was quite consistent: the disconnect between health care and social services frustrated them. Was this surprising?
LT: We asked these providers about their experiences at the front lines: what kind of interactions they had with each other, how their work crossed the boundary between the two sectors, and what challenges exist in working across that boundary. How does the current system support them in that cross-boundary work, or how does it impede them in that sort of thinking?
Having done qualitative work before, we're used to really having to dig to pull out these emergent themes that fit the data set. But here, it was just so clear. People said on both sides ,"Yes, we're treating the same populations, and it's incredibly frustrating to feel like I don't have contact with people who work in the other sector."
EB: It was clear as a bell that we were capturing something that was already ingrained in the experience of front-line providers. There's sort of a moment in time with the ACA, among other things, that may put us on a platform to really shift in how we think about health care and our investment in health.
My caution is that we've been here before. There have been times — in the late '60s, the early '70s, the '90s — where the country put together plans and legislation to try to make providers think about the social determinants of health. And each time, through complicated cultural, economic, and social pressures, we have veered back into our comfort zone of medicalization.
I'm eager to watch what's happening right now, but if history is predictive, it's possible we'll go right back down that road.
AM: What are some of the most important lessons we can take away from other nations on how to bridge this gap between health care and social services?
EB: I would pick out three lessons. The first is that a lot of our current situation is related to root cultural values underlying the history that has brought us to this place.
Looking elsewhere, we thought the ideas in Scandinavia were very interesting. But can we really staple those into the United States? Maybe not, because it's not just the strategy they're using today; that strategy is sitting on a historical bedrock of greater collectivism. Culture and underlying values are pieces of this puzzle.
The second lesson is perhaps less depressing. There are interesting tactics that have been used in other countries that I think we can do something with. For example, one that I think is most important is joint budgeting and joint planning for both health services and housing, education, employment support, and other social services. This is something we saw again and again in Scandinavia, and it makes sense. It forces people to say, "Here's all of the money we have to spend, here are all of the services we could get. How can we maximize the impact on health?"
We don't do that in the United States. We could, but we don't.
The last lesson is maybe the most hopeful. While Scandinavian nations are often seen by the United States as very socialized, the truth is that they run on localism. All of this joint budgeting and planning happens at a local, county level. That gives great hope to the United States that there can be great experimentation at the local level.
There's a huge amount of potential for the private sector to be quite innovative with this, and I'm really excited to see what they do. I do have some pause because the money and the previous responsibility has always been with the health care sector; it seems natural for them to take a leadership role. What's the balancing force that will ensure that that leadership doesn't tip us back into the medicalization problem? That will be our challenge.
LT: In Scandinavia, there's a sense of accountability for population health at the local level. I think that's part of the concern here. In Scandinavia, the local government really takes the lead and they're the arbiter of different interests. They make sure the process is moving forward, and that the planning and the budgeting is responsive to public needs.
Who's going to play that role in the United States? Someone needs to hold the reins. In Scandinavia, it's very clear who should lead. Here, we're not really sure who plays that role.
AM: I know you don't presume to have all of the answers for solving our health care system's problems, but what should we look to do in the short term? What are some immediate next steps that we can point policymakers toward?
LT: The excitement around the "culture of health" concept and shared accountability is fantastic. We're so pleased to see it, and to see so many big names and big funders coming on board. The fear that I have in that is that "culture of health" will become a piece of jargon and the health economists will roll their eyes and dismiss it as "fluffy" or pie-in-the-sky.
I think the research agenda should move quickly to identify a few things: who will lead, how will accountability be measured, and what are the metrics of shared accountability or integration across structural boundaries that we want to be testing in a rigorous empirical way.
EB: We also really need to change the dialogue for "everyman" on the street. We need to promote an actual understanding of what creates health and how dangerous it can be — and how expensive it can be — to not pursue the most effective things to promote health. To have that more in the fabric of everyday life in America, that's what's needed.
AM: Something you explore in your book that I haven't seen much elsewhere is trying to understand why our welfare system looks so much different than that of other nations. I thought you put forward a really interesting theory about how the USdoesn't have a history of feudalism that many other nations share.
LT: This hypothesis came from some of the interviews we did in Scandinavia, where we asked people why they thought their nations had such confidence and trust in government. We would joke with them about Reagan and how he said the nine most frightening words in the English language are "I'm from the government and I'm here to help." They would just kind of giggle and say "We have none of that attitude here."
When we pressed some people on why they think that is, this emerged. For them, the state has just been around for so long and has always been seen as a provider.
The government grew out of a feudalist system where the feudal lords really had an interest in caring for people we might call "serfs." The underprivileged were seen as an integrated part of the economy. There was an interest on the part of those who had means to care for those who didn't.
There's another interesting hypothesis that is somewhat connected to this: they don't have a very vibrant church community in Scandinavia. There was never this organic religious community to spawn a nonprofit system where responsibility for the underserved could be outsourced. The state could not be let off the hook in that way.
These are hypotheses, but they're historically grounded — it's interesting to think about how deep some of these attitudes toward government can run.





